Pneumothorax involves collapsed lungs with air filling the space that surrounds the lungs within the chest cavity. Pneumothorax cases with severely collapsed lungs are potentially life-threatening, especially if the accumulation of air in the chest cavity is rapid and progressive leading to the ever-increasing pressure on ever collapsing lungs (tension pneumothorax). Pneumothorax cases typically fall into two groups.
The first group, comprising most of the cases that we see, involves trauma, usually follows road traffic accidents, where broken ribs etc leads to a punctured lung or damaged airway. The punctured lung (or airway) is where the air that fills the chest cavity comes from. Occasional cases involve external trauma like bite wounds where big dogs maul little dogs, although many of these cases would not survive long enough to get veterinary attention. The canine teeth of the large dog penetrate the chest cavity and air can enter the chest cavity through the wound, without having first gone down the airway into the lungs. Surgical interventions where external air has the opportunity to enter the chest through a chest wall wound or through a hole in the diaphragm would also fall into this category of traumatic pneumothorax. This first traumatic pneumothorax group can usually be treated by keeping the lung cavity drained for a few days while any tear in the lung seals over, or while any chest wall wound heals. Damaged airways sometimes need to be surgically repaired. Minor volumes of pneumothorax in clinically stable animals can sometimes be left to resolve spontaneously without intervention.
The second group of pneumothorax cases involves pathological areas of lungs that then rupture and allow air to accumulate in the chest cavity. The lungs in these cases does not usually heal over and the affected area of lung usually needs to be removed surgically. So long as the affected area is localised the prognosis following removal of a lung lobe is usually good.
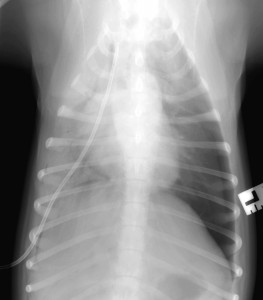
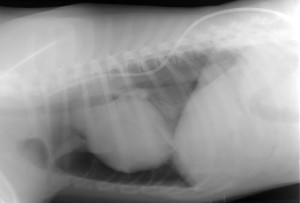
Vesper was a young Labrador, hit by a car. There was respiratory distress (difficulty breathing). Conscious X-rays are rarely of as good a quality as is possible under GA, but if the patient will remain still for a moment under the X-ray beam, they are usually plenty adequate to get a “handle” on what is going on. Vesper obliged, and a conscious X-ray showed the collapsed lungs and air surrounding the lungs within the chest cavity. The question was then whether to sedate or anaesthetise to get control of the situation. A dog that has had trauma and pneumothorax is not a standard anaesthetic risk. On the other hand, once under anaesthetic with a tube placed in the trachea (windpipe), we could ventilate the lungs artificially. Under sedation with no tracheal intubation in place, we were reliant on Vesper continuing to ventilate her own lungs. We hedged our bets and went for sedation, with everything to hand for immediate anaesthetic induction and/or emergency intubation if her oxygen levels crashed. A chest drain was placed into the chest cavity through the right chest wall. Once the air was removed from her chest cavity and the lungs re-inflated, her breathing markedly improved. X-ray (still conscious so still less than perfect positioning!) confirmed the position of the drain. Sometimes the drains are a bit of a law unto themselves and can fold into curious positions within the chest cavity, but this one was lying nice and straight. Sometimes the (which divides the two halves of the chest cavity) prevents a chest drain on one side from draining the other side too. But in this case, one drain sufficed to drain both sides and there was no need to place one on the other side as well.
In the post-op period after chest drain placement, it is essential to have “eyes on” the patient. If the chest drain is interfered with, air can flood back into the chest cavity and the patient is right back into a life-threatening scenario. We secure the drain to the side of the chest with a skin suture and with a Tubigauze vest, and an Elizabethan collar is used.
Vesper was amazingly happy and contented and seemed utterly unconcerned by the presence of the injury of the drain. 100-200ml of air was being removed from her chest every 30-60 minutes via the drain and a suction system. This volume gradually declined over the next 48 hours. Chest drainage and close observation was continued through the night in Burton-Upon-Trent. Once the volume was down to just a few ml of air, (and a few ml of fluid, which is actually caused by the drain itself, acting as a foreign body), we removed the drain. Vesper was discharged from us at West Midlands Veterinary Referrals for strict rest at home for the next 2-3 weeks while the sealed tear in the lungs reliably repairs.
3rd October 2015